

The NHS: Where does all the money go?
The NHS: Where does all the money go?
Part 4: NHS England (overview)


We continue our walkabout the English NHS following the wiring diagram presented to Parliament.

Body name NHS England
Place in the wiring National body
The body's stated function is to lead the National Health Service (NHS) in England.
Its budget of GBP 153 billion was reported in Parliamentary accounts. According to the Accounts included in the NHS England annual report and accounts for 2022-23, it is GBP 157 billion.
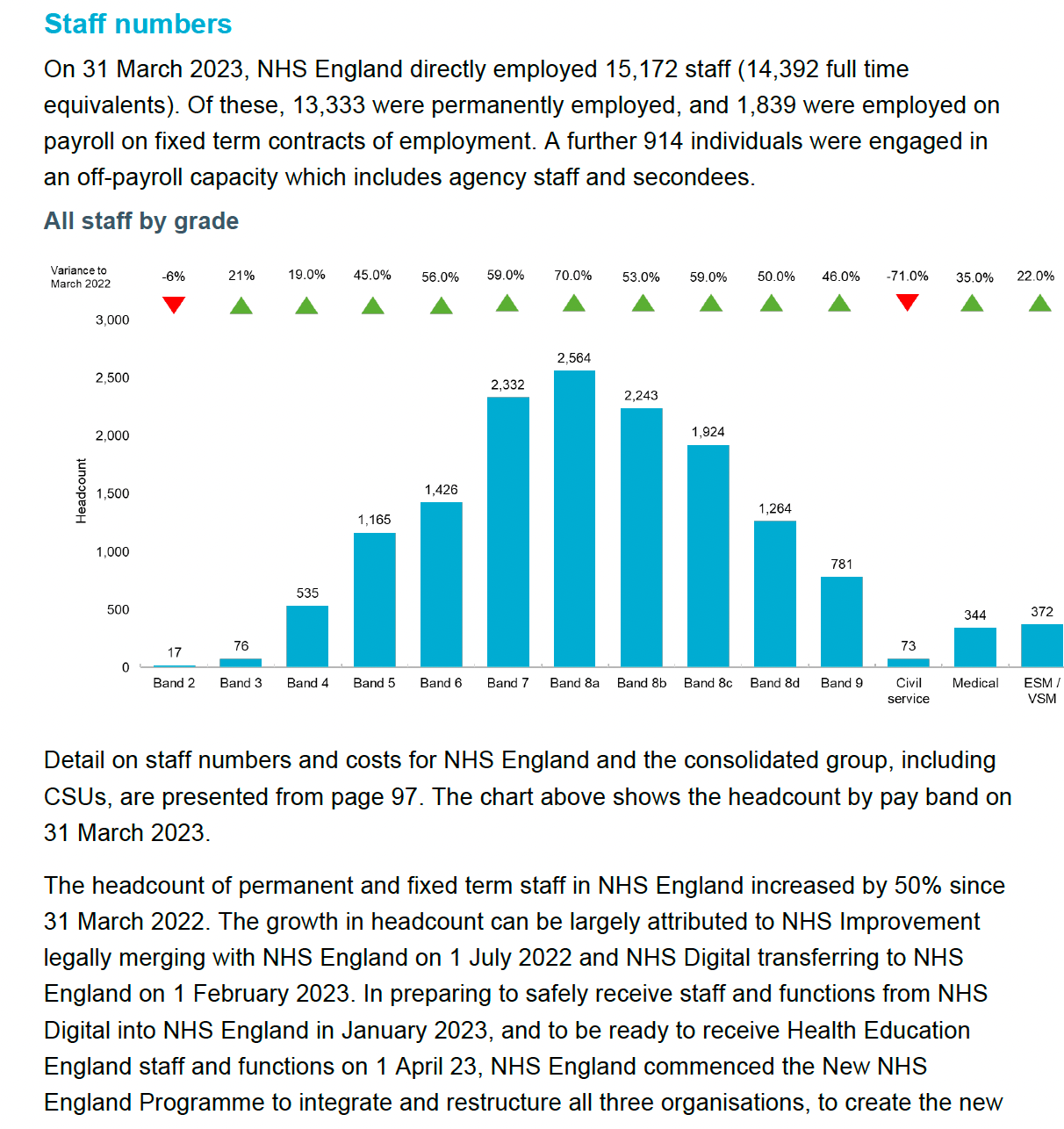
According to Wikipedia. NHS England had 6,500 employees in 2021. Another source puts the number at over 10,000. The Report cites on page 88:
The report also shows that 1,078 people agreed to exit packages in 2022-23 that cost GBP 79 million (See page 104).
Of note, 40 people got exit packages worth more than GBP 150,000.
The top salary in 2022-23 was Chief Executive Amanda Pritchard’s— GBP 255,000 to 260 (page 106). However, Ms Pritchard also received up to GBP 72,50 in pension contributions, taking her total salary to GBP 330,000.
In 2022-23 (page 116), NHS England accounted for GBP 56.4 Million of losses and special payments. These are payments that Parliament would not have known about when agreed funding levels and “ideally should not arise” (page 116).
Patient/societal benefit from the function to be defined
Grey areas: We started looking from the top of the NHS England pyramid. So, we decided to start with the Board members and their disclosure declarations, which are available here. We leave it to our readers to comment on the makeup of the Board and members’ baggage. Bear in mind that family members' interests are disclosed, too.
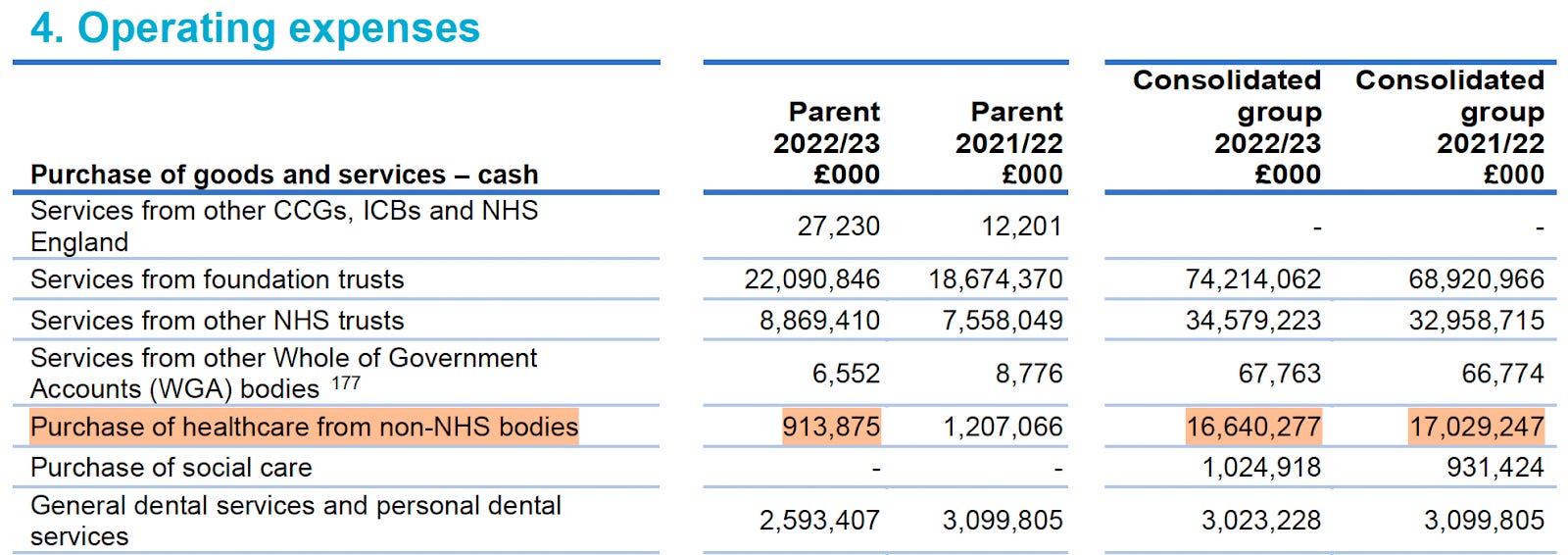
Readers may wonder why an organisation like the NHS, which employs 1.5 million people, should spend £16.6 billion to purchase care elsewhere.
Recommendations or comments
The website is busy, with an alphabetical index of activities or topics. Consequently, the current post is an umbrella or signpost to which we will add further information, updating the post as we go along. Also, if we identify entities directly linked to NHS England or parts of it, we will cover them as 6a, 6b, etc., as we did with the Comirnaty series to indicate each post’s lineage.
Two old geezer taxpayers wrote this post and are finding difficulties keeping track of the naughts.
Could it be agency costs?
Looking back over the last 10y, the DDRB uplift /pay 'award' to UK general practices were:
0% 2012
1% 2013
0% 2014
0% 2015
1% 2016
1% 2017
3% 2018
3% 2019
2.95% 2020
4% 2021
5% 2022
6.5% 2023
So significant erosion of income in the austerity years with increased inflationary costs year on year. In that time the complexity and the volume of the work mushroomed, more work absorbed from secondary care and with an ageing and increasingly metabolically unhealthy population. More expected for less.
Many left the profession to retire early, earn higher wages through career change, agency/locum work, work abroad, private practice or to free themselves of the suffocating bureaucracy that can be associated with substantive NHS posts (including CQC generated targets). Clinicians moved into private practice or moved to 'portfolio careers' (part time working in the NHS) as they can earn more and engender more respect and patient satisfaction when access and continuity of care is no longer an obstacle. Some work from home. Some services like psychiatry seem to be entirely run by a transient locum consultant workforce.
Shifts need to be covered when staff leave. In some areas, workers learn that last-minute shifts attract a higher premium, so this compounds the problem of cost (why volunteer for an out of hours shift months in advance when you could agree to it last minute and earn double the income?). Agency costs have mushroomed as the workforce becomes increasingly fragmented and disjointed:
https://www.rcn.org.uk/news-and-events/news/uk-32bn-agency-spend-could-have-paid-salaries-of-31000-nurses-051223
https://www.theguardian.com/society/2024/jan/16/nhs-across-uk-spends-a-staggering-10bn-on-temporary-staff
https://www.bbc.co.uk/news/world-europe-guernsey-65028287
Meanwhile, NHS nurses and health workers in some areas have resorted to using food banks.
In primary care, unlike private businesses, the GMS contract limits the ways that GP practices can increase practice income. Income earned through 'enhanced services' (minor surgery etc) has been eroded (with 0% inflationary adjustments over a decade), effectively meaning provision of some services come at a loss so practices stop providing. Other 'enhanced service' work became so bureaucratised it created significant extra work with uncertainty about value (eg payments for dementia 'case finding' rather than waiting for people to present with dementia concerns). less time available for the stuff that makes a difference but which doesn't pay extra. Some practices have moved into 'research' to supplement practice income, achieve stability of income and attract staff. Pharmaceutical industry sponsored research is higher paying but also introduces conflict of interest.
There is a tipping point when more and more people choose to leave stable substantive posts (eg partnerships, or even salaried posts), citing reasons of work-life balance, pay and self-protection (mental health).Continuity of care suffers and there is more waste as it takes twice as long to get to the bottom of a problem when no-one takes ownership or when a service doesn't exist any more. For those who remain, this adds more and more stress for increasing financial penalties and facing and increasingly dissatisfied public.
In 2017 there was an election promise to spend an extra £8 billion on the NHS over 3 years and a lot of fuss was made about that, as if it was a great gift after so many years of cuts. And then in 2020 suddenly the coffers were opened again, money was no object and the government began burning its way through obscene amounts of public money in the name of Covid. As an example, by December 2021 they had spent more than £16.6 billion on lateral flow rapid antigen tests (9.5% of the NHS budget or 1.4 x the annual NHS primary care budget equivalent on a single test) and £37 billion budget for NHS test and trace.
And yet the public in general did not question any of this as they squirrelled away these 'free tests' and demanded more to keep them safe as the NHS finally imploded. In the end the NHS broke the NHS in the pandemic years, but it was in very very bad shape already.
Not sure I can continue reading these figures without feeling sick and my blood pressure rising!