
Wiser Healthcare
Excessive Testing and Braess’s paradox in healthcare


Ministers have fallen in love with diagnostics: more scans, more blood tests, more pathways and more community diagnostic centres. They boast of capacity expansion as though healthcare were merely an engineering problem requiring wider pathways and faster throughput. Wes Streeting recently hailed the government’s programme as “the biggest expansion in NHS diagnostics in a generation.”
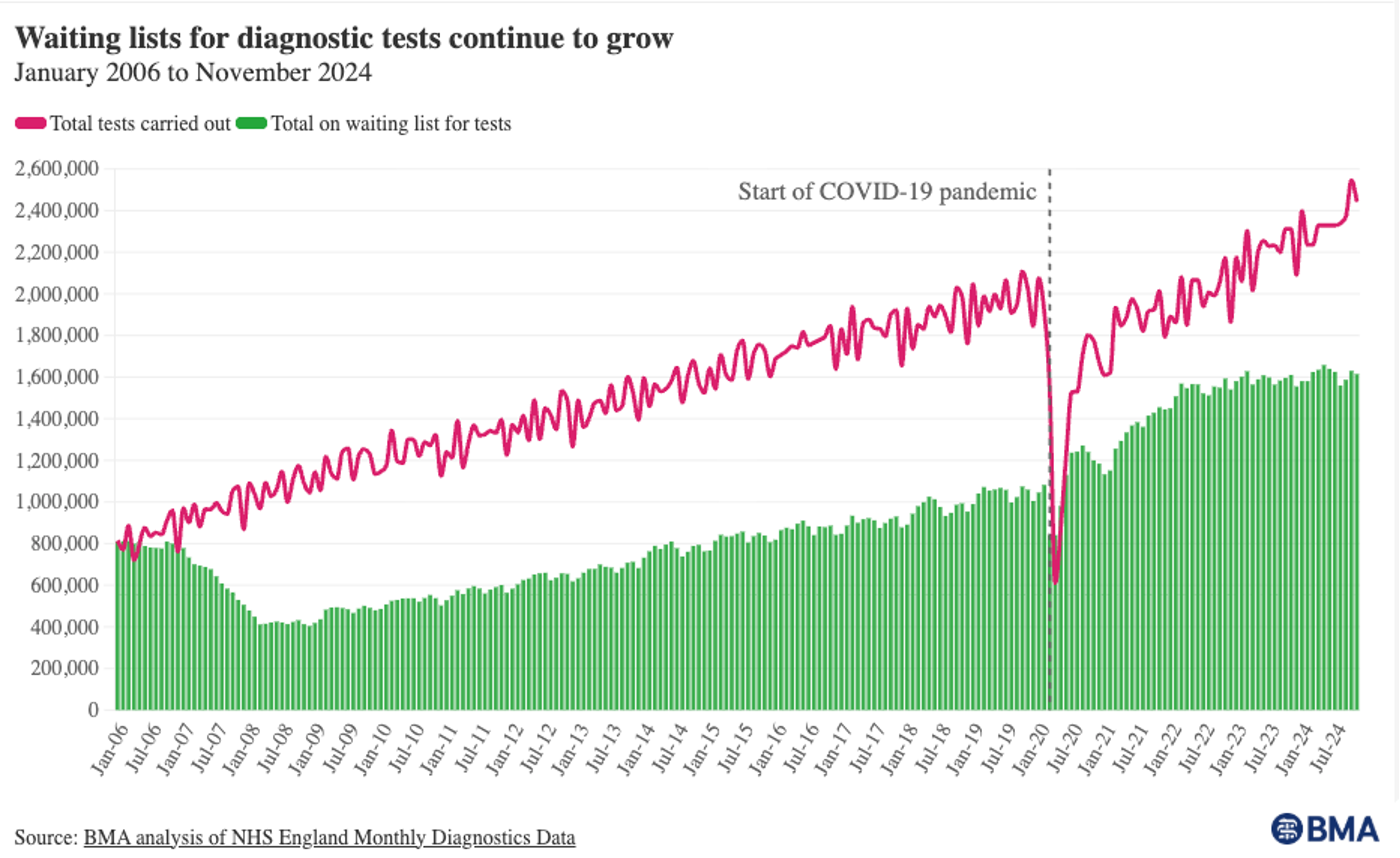
Yet after two decades of relentless growth in testing, waiting lists continue to rise, clinicians are drowning in results, and patients remain stuck in the system.
Transport economists recognised this decades ago. Build another motorway lane, and congestion often returns; in some cases, it worsens. The phenomenon is known as Braess’s paradox: induced demand and extra capacity change behaviour. People make journeys they previously avoided, they travel farther, or drive at busier times, and the new road fills up.
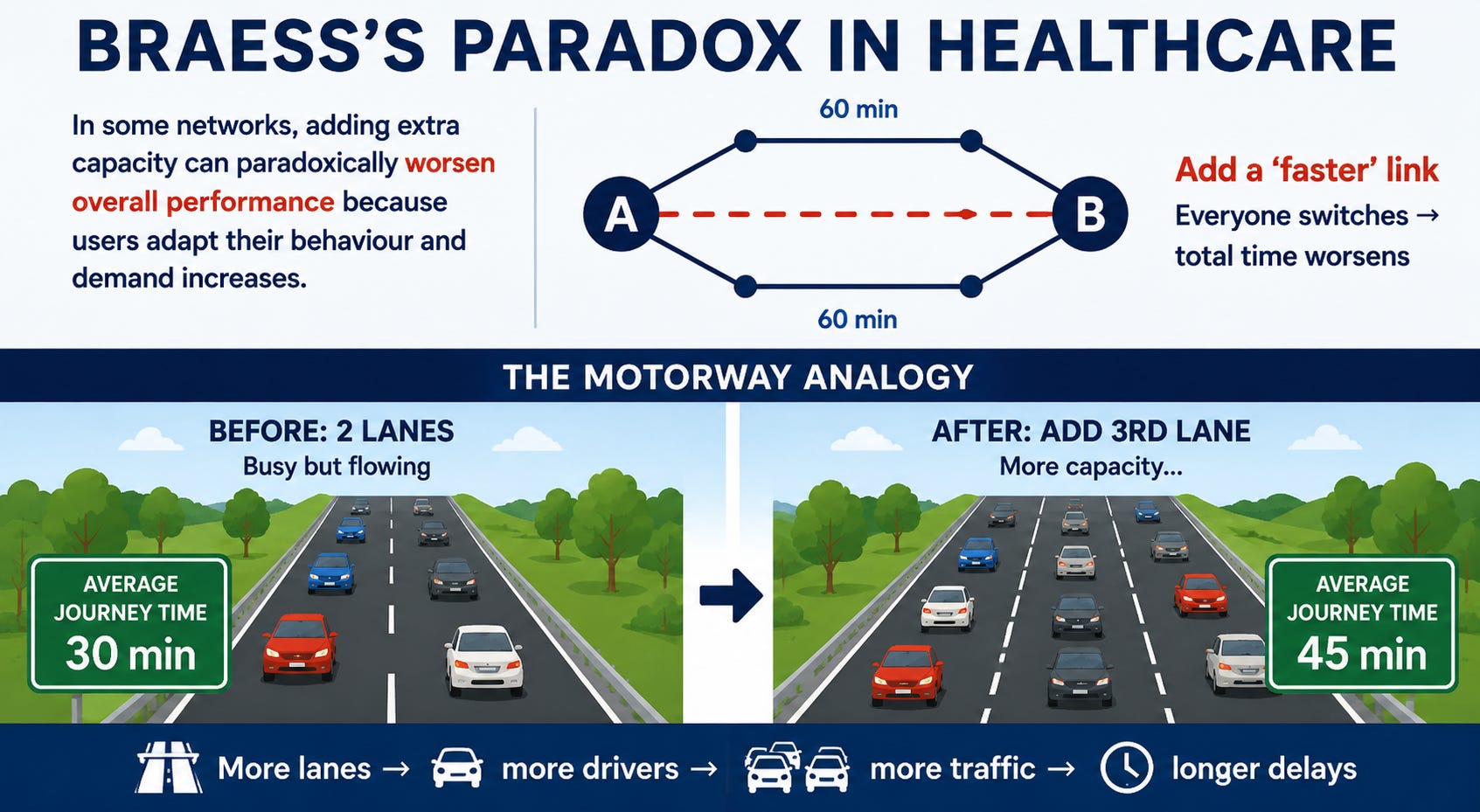
Healthcare is now experiencing its own version of Braess’s paradox.
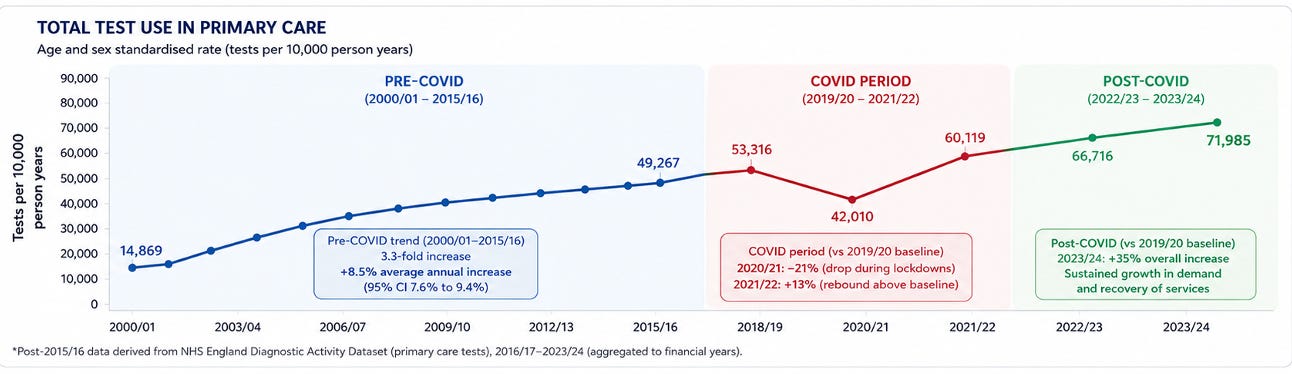
Our research found that NHS primary care testing increased 3.3-fold between 2000 and 2015, from around 15,000 tests per 10,000 person-years to nearly 50,000 tests per 10,000 person-years. Patients averaged five tests per year by 2015, compared with 1.5 in 2000. Since then, the trend has accelerated post-COVID, with expanding access to diagnostics, community testing centres and direct GP access to imaging.
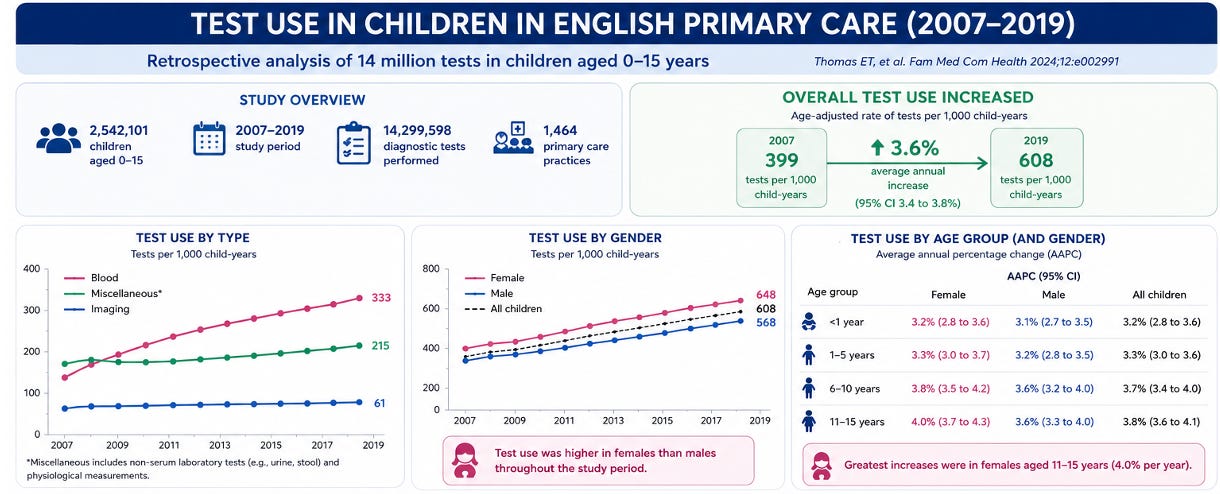
Children have not escaped the trend either. Our research also showed that paediatric testing in English primary care rose steadily between 2007 and 2019, driven particularly by blood tests in adolescent girls and increasing testing in deprived populations. Vitamin D testing, faecal calprotectin and nitric oxide testing showed extraordinary increases.
Yet despite this explosion in diagnostic activity, the system feels more congested than ever.
Why?
Because more capacity does not simply process existing demand, it creates new demand.
The threshold for testing falls; clinicians become more risk-averse, and patient expectations for investigations rise. Guidelines increasingly favour “rule-out” strategies, and defensive medicine is entrenched as diagnostic testing feels safer than observation.
Every new test also creates downstream traffic. A blood test does not end with the needle; it generates interpretation, repeat monitoring, referrals, follow-up imaging, incidental findings and specialist appointments. One scan begets another. A mildly abnormal result triggers surveillance, and a harmless incidentaloma becomes a lifelong medical identity.
The system then behaves like a motorway network where every new junction feeds congestion further downstream.
The NHS’s latest answer is Community Diagnostic Centres. In 2022, the Government announced more than 160 CDCs to expand access to MRI, CT, ultrasound and endoscopy. Nearly 170 are now operational.
The policy logic is understandable, but there is an uncomfortable paradox at the heart of this strategy: The easier diagnostics become, the more they are used.
The result is visible everywhere with reporting delays, workforce shortages and growing waiting lists. More than one in five patients still wait over six weeks for diagnostics despite record activity levels. The bottleneck has merely moved downstream — from obtaining the test to interpreting and acting upon it.
Now ministers increasingly place their hopes in artificial intelligence. AI-assisted radiology, automated pathology, algorithmic triage systems and GPT-style decision support are all presented as solutions to the productivity crisis.
AI will undoubtedly help in some areas. It may improve image interpretation, prioritise abnormal scans, reduce reporting times and support probabilistic reasoning. One recent JAMA study found that GPT-4 outperformed clinicians in several tasks involving estimation of diagnostic probabilities after negative test results.
But AI risks intensifying the paradox.
If diagnostics become faster, cheaper and easier, clinicians may simply order more of them.
Why not request another scan if the report is generated instantly? Why tolerate uncertainty if AI can “just check”? Lower friction often means lower thresholds as the healthcare motorway gains another lane — and more traffic pours in.
There is also a greater danger. AI systems may be statistically sophisticated, but healthcare is not merely a pattern-recognition exercise. Diagnosis requires judgement about uncertainty, context and consequences. The Rodman study showed that AI still struggled in some positive-test scenarios and could misinterpret clinical framing. In the real world, over-reliance on AI risks amplifying automation bias, incidental findings and unnecessary cascades of care.
Too often, policymakers assume that more diagnostics automatically mean better healthcare. Yet a good test is not one that simply produces more information. A good test narrows meaningful uncertainty and changes management in ways that benefit patients.
That distinction matters enormously.
Healthcare systems do not fail because they lack activity; they fail because they generate activity faster than they can absorb its consequences.
Unless we confront the culture of excessive testing, no amount of scanners, CDCs, or AI will truly solve the congestion crisis. We will simply become more efficient at producing bottlenecks.
Two old geezers wrote this post who think the healthcare system could do with a little more wisdom and a little less activity.
This piece originated as a talk given in Oxford on excessive testing, diagnostic capacity and Braess’s paradox in healthcare. It draws on a programme of research examining rising diagnostic activity in UK primary care, including the work of Dr Elizabeth Thomas and Dr Jack O’Sullivan, whom Carl supervised at the Centre for Evidence-Based Medicine, University of Oxford. Their studies explored the rapid growth in adult and paediatric testing, the variation in clinical practice, and the downstream consequences for workload, costs and patient care.
Below the waterline, you can access Carl’s talk.
